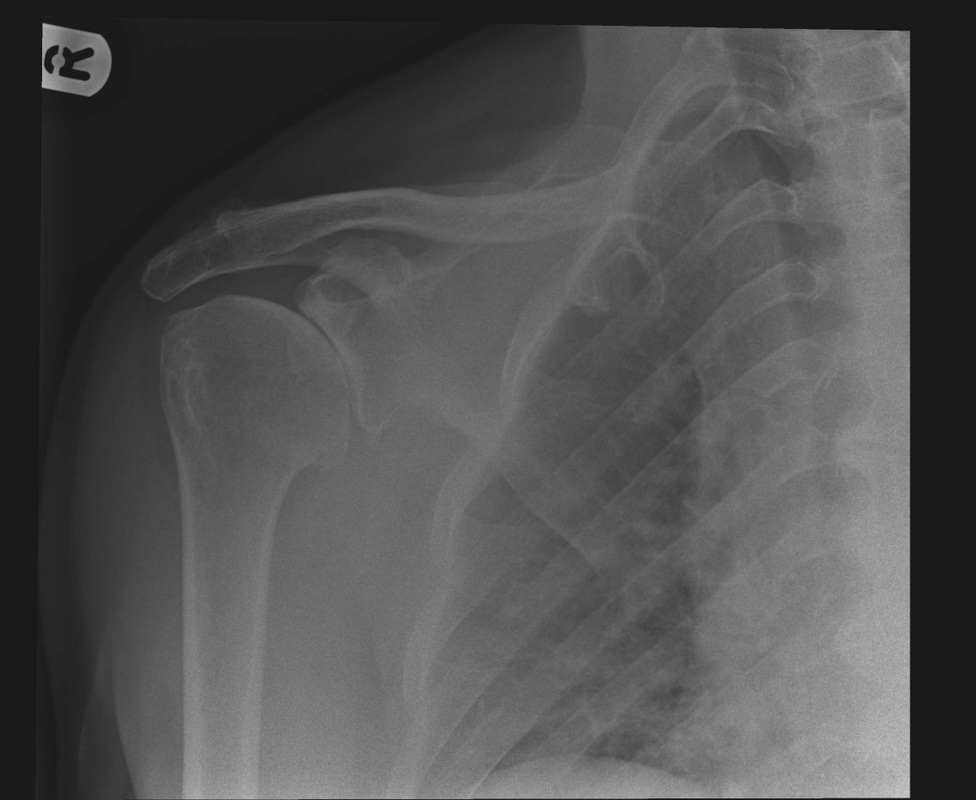
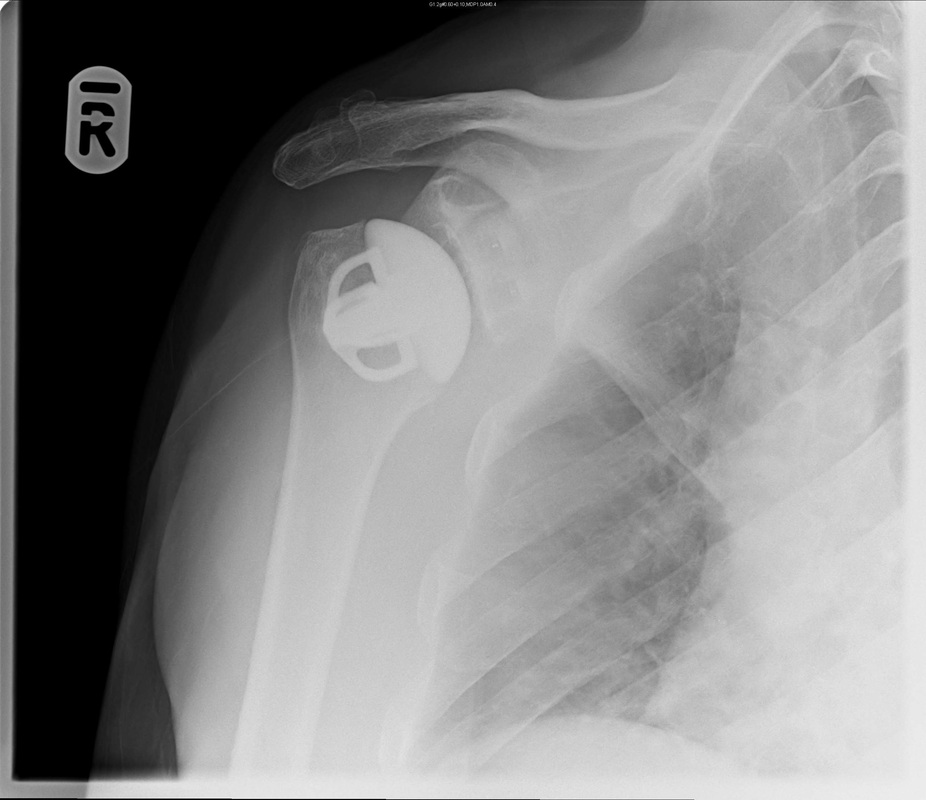
Arthritic shoulder Post Short Stem Shoulder Replacement
A Typical Patient Experience
The patient was seen in clinic where he presented with a generalised aching pain in his shoulder and reduced and painful movements.
Following a plain X-ray of his shoulder that day he had a further discussion with Mr Hamlet who explained that the X-rays showed decreased joint space and osteophytes around the edge which suggested that the reason for the pain and stiffness was an arthritic shoulder joint.
Options such as pain treatment with tablets or steroid injections and physiotherapy were discussed and it was decided that the most appropriate treatment woulfd be a shoulder replacement
The patient chose a date that suited him best and arrived at the hospital in the late afternoon for operation that evening
He was admitted to the ward by the nursisng staff and then seen on the ward by the consultant surgeon ( mR Hamlet) and the consultant anaesthetist. They reconfirmed exactly what was planned. He then had an arrow placed on his arm and went to theatre
In the anaesthetic room in theatre he had a fine needle inserted at the base of his neck, under ultrasound control (See Dr Bhatti page for image) to insert a local anaesthetic to numb the arm
He was then put to sleep.
The next thing he remembers is waking up in the recovery with no pain and a numb arm that didn't move.
He went back to the ward shortly after and was able to eat and drink. The next morning he was comfortable, the feeling had returned to the arm and he went home wearing a sling (if operations are done earlier in the day then patients may go home on the same day)
Two weeks later he returned to the clinic. He was taking no painkillers for the shoulder, he was occasionally using the sling but was using the arm for gentle activities. He had a further X-ray (see above)
He has been told that over the next 2-3 months he should expect to get back to most activity but it will be 18 months before he can expect no further improvement
The patient was seen in clinic where he presented with a generalised aching pain in his shoulder and reduced and painful movements.
Following a plain X-ray of his shoulder that day he had a further discussion with Mr Hamlet who explained that the X-rays showed decreased joint space and osteophytes around the edge which suggested that the reason for the pain and stiffness was an arthritic shoulder joint.
Options such as pain treatment with tablets or steroid injections and physiotherapy were discussed and it was decided that the most appropriate treatment woulfd be a shoulder replacement
The patient chose a date that suited him best and arrived at the hospital in the late afternoon for operation that evening
He was admitted to the ward by the nursisng staff and then seen on the ward by the consultant surgeon ( mR Hamlet) and the consultant anaesthetist. They reconfirmed exactly what was planned. He then had an arrow placed on his arm and went to theatre
In the anaesthetic room in theatre he had a fine needle inserted at the base of his neck, under ultrasound control (See Dr Bhatti page for image) to insert a local anaesthetic to numb the arm
He was then put to sleep.
The next thing he remembers is waking up in the recovery with no pain and a numb arm that didn't move.
He went back to the ward shortly after and was able to eat and drink. The next morning he was comfortable, the feeling had returned to the arm and he went home wearing a sling (if operations are done earlier in the day then patients may go home on the same day)
Two weeks later he returned to the clinic. He was taking no painkillers for the shoulder, he was occasionally using the sling but was using the arm for gentle activities. He had a further X-ray (see above)
He has been told that over the next 2-3 months he should expect to get back to most activity but it will be 18 months before he can expect no further improvement
